PMOS is a Metabolism Problem: Why This Changes Everything
PMOS is a metabolism problem, not an ovary problem. Here is why that distinction changes how Indian women are diagnosed, treated, and how real Indian food can address the root cause, not just the symptoms.

Table of Contents:
1. Why the Old Name Created a Dangerous Misunderstanding
2. What PMOS Actually Is: A Metabolic and Endocrine Condition
3. The Insulin Resistance Engine: How It Drives Everything Else
4. The Full-Body Impact of PMOS
5. Why Indian Women Are Disproportionately Affected
6. What the Metabolic Framing Means for Treatment
7. How Real Indian Food Addresses the Root Cause
8. What You Can Do Right Now
9. Conclusion
10. FAQs
Why the Old Name Created a Dangerous Misunderstanding
PMOS is a metabolism problem — and the fact that it was named after ovarian cysts for decades is one of the most consequential errors in women's health. The name PCOS, Polycystic Ovary Syndrome, directed every doctor's attention toward the ovaries. And for millions of women, that meant the real problem was missed entirely.
The Name That Misdirected Treatment for Decades
Here is the fundamental error: women with PCOS do not necessarily have ovarian cysts. Research published alongside the PMOS rename in The Lancet confirmed there is no increase in abnormal ovarian cysts in the condition. The cysts were a byproduct, not the cause. The cause was always metabolic.
When doctors looked at the ovaries and saw nothing dramatic, women were told their symptoms were hormonal, that they needed the pill, or that they just needed to lose weight. The insulin resistance driving everything in the background was rarely tested for and almost never treated first.
What the PMOS Rename Acknowledges
The rename to PMOS, published in The Lancet on 12 May 2026 and endorsed by 56 global organisations, makes one thing clear: this is a complex, multi system condition involving endocrine, metabolic, reproductive, dermatological, and psychological health. Not a gynaecological problem. Not a fertility problem. A whole-body metabolic condition.
That shift in framing is not semantic. It changes what tests should be ordered, what treatment should look like, and most importantly, what food should do for you.
What PMOS Actually Is: A Metabolic and Endocrine Condition
PMOS is a metabolism problem that sits at the intersection of three interconnected systems: the endocrine system, the metabolic system, and the reproductive system. Each one influences the others. You cannot fix one without addressing all three.
The Three Systems in PMOS
The endocrine system: Multiple hormones are dysregulated simultaneously. Insulin, androgens (male hormones), LH, cortisol, and in many women, thyroid hormones. This is why the new name includes the word polyendocrine. It is not one hormone. It is a hormonal cascade.
The metabolic system: Insulin resistance is present in up to 85% of women with PMOS, including 75% of lean women with a BMI below 25. This means the metabolic disruption is not about weight. It is about how cells process glucose and respond to insulin signals.
The reproductive system: The ovaries are affected, but downstream. Excess insulin signals the ovaries to produce more androgens. Those androgens disrupt the follicle maturation process. Irregular periods and fertility challenges are a consequence of the metabolic and endocrine disruption, not the source of it.
Why This Distinction Matters for Every Woman With PMOS
If the problem starts in metabolism, the solution starts in metabolism. Not in the ovaries. Not in the uterus. In how your body processes glucose, manages inflammation, and balances the hormonal cascade that begins with insulin.
This is where food becomes the most powerful tool available. And this is the foundation of how we work at Fuel It Right. Every protocol we build starts with the metabolic root, not the reproductive symptom. More on that in Section 7.
The Insulin Resistance Engine: How It Drives Everything Else
Understanding PMOS as a metabolism problem requires understanding insulin resistance. It is the engine running almost everything you experience with this condition.
Here is the cascade, step by step:
• Cells stop responding properly to insulin. Blood glucose stays elevated after meals.
• The pancreas compensates by producing more insulin. Hyperinsulinaemia develops.
• Excess insulin signals the ovaries to produce more androgens (testosterone, DHEAS).
• Elevated androgens disrupt follicle development, causing irregular or absent ovulation.
• High androgens drive acne, excess facial and body hair, and scalp hair thinning.
• Chronic high insulin drives fat storage, particularly visceral fat around organs.
• Visceral fat produces inflammatory signals that worsen insulin resistance further.
• The cycle deepens.
The number that reframes everything Insulin resistance is present in 85% of all women with PMOS and in 75% of lean womenwith PMOS whose BMI is below 25. This is not a weight problem. This is a cellular problem. And it responds directly to how, what, and when you eat. |
What Insulin Resistance Feels Like Day to Day
Most women with PMOS describe the same cluster of experiences without connecting them to insulin. Fatigue after meals, especially after rice or roti. Intense sugar cravings at 3pm. Difficulty sleeping. Brain fog. Slow weight gain over years despite no obvious change in eating. Morning stiffness and bloating.
These are not separate problems. They are one insulin problem presenting in different tissues.
The Full-Body Impact of PMOS
PMOS is a metabolism problem that shows up across every system in the body. This is what distinguishes it from a simple hormonal condition and why treating only the periods or only the fertility rarely works.
Skin | Acne along the jaw and chin, darkening of the neck and underarms (acanthosis nigricans), and skin tags are all driven by insulin resistance and androgen excess. These are metabolic signs, not cosmetic problems. |
Hair | Scalp hair thinning and unwanted facial or body hair are androgen-driven. They will not resolve until androgen levels come down, which requires addressing the insulin resistance driving them. |
Gut | PMOS significantly disrupts the gut microbiome. Women with PMOS have measurably lower levels of beneficial bacteria, higher intestinal permeability, and higher circulating inflammatory markers. The gut-hormone connection runs both ways. |
Mental health | Anxiety and depression are significantly more prevalent in women with PMOS, independent of weight or fertility concerns. The hormonal and inflammatory disruption directly affects neurotransmitter production and mood regulation. |
Heart | Long-term elevated insulin, cholesterol, triglycerides, and blood pressure all increase cardiovascular risk substantially. PMOS is now classified as a cardiometabolic condition, not just a reproductive one. |
Thyroid | Co-occurrence with hypothyroidism is significantly higher in Indian women with PMOS than the global average. Both conditions affect metabolism, weight, energy, and cycles — and each one worsens the other if untreated. |
Why Indian Women Are Disproportionately Affected
PMOS as a metabolism problem hits Indian women harder than the global average. Roughly 1 in 5 Indian women of reproductive age has PMOS, compared to 1 in 8 globally. The reasons are specific and important.
The South Asian Metabolic Profile
South Asian women carry significantly more visceral fat, which is fat stored around internal organs, at the same BMI as women of other ethnicities. A woman at a BMI of 23 may carry the metabolic fat profile of a European woman at BMI 27. This means insulin resistance develops earlier, at lower body weights, and with fewer external warning signs.
Layered on top of this genetic predisposition is a daily diet built predominantly around refined carbohydrates. White rice, maida rotis, biscuits, sweetened chai, packaged snacks. Every one of these drives glucose spikes and insulin surges that, over time, deepen insulin resistance.
The Thin Woman Problem
Because PMOS was historically framed as a weight condition, lean Indian women were routinely dismissed. If you do not look overweight, you were told you could not have PCOS. But 75% of lean women with PMOS have insulin resistance. The problem is cellular, not cosmetic. If you have been dismissed because of your weight, ask your doctor for a fasting insulin test and a HOMA-IR calculation.
What the Metabolic Framing Means for Treatment
If PMOS is a metabolism problem, then the first line of management must target metabolism. This is a significant departure from how most women with PCOS were treated under the old framework.
What Was Often Done Before
• Oral contraceptive pill to regulate periods.
• Metformin for insulin resistance, rarely explained to patients.
• Weight loss advice without addressing the root metabolic cause.
• Fertility treatment when conception was the immediate goal.
• Symptomatic treatment of acne, hair fall, and skin changes.
None of these are wrong. Some are genuinely useful. But they were applied without the metabolic foundation, which is why so many women cycled through treatments without addressing the actual condition.
What the PMOS Framework Prioritises
• Fasting insulin and HOMA-IR as primary diagnostic markers, not optional additions.
• Metabolic management as the first and central intervention.
• Food as the primary therapeutic tool, not an afterthought.
• Gut health as a co-target, given the microbiome-hormone relationship.
• Thyroid screening as standard, not reactive.
• Mental health support as part of the protocol, not separate.
The question that changes the consultation The old question was: how do we manage your symptoms? The new question is: how do we restore your metabolic function? That shift changes everything from which tests are ordered to what you are asked to eat for breakfast. |
How Real Indian Food Addresses the Root Cause
PMOS is a metabolism problem that responds directly to food. Not supplements. Not detox teas. Not elimination diets. The right food, in the right combination, at the right time.
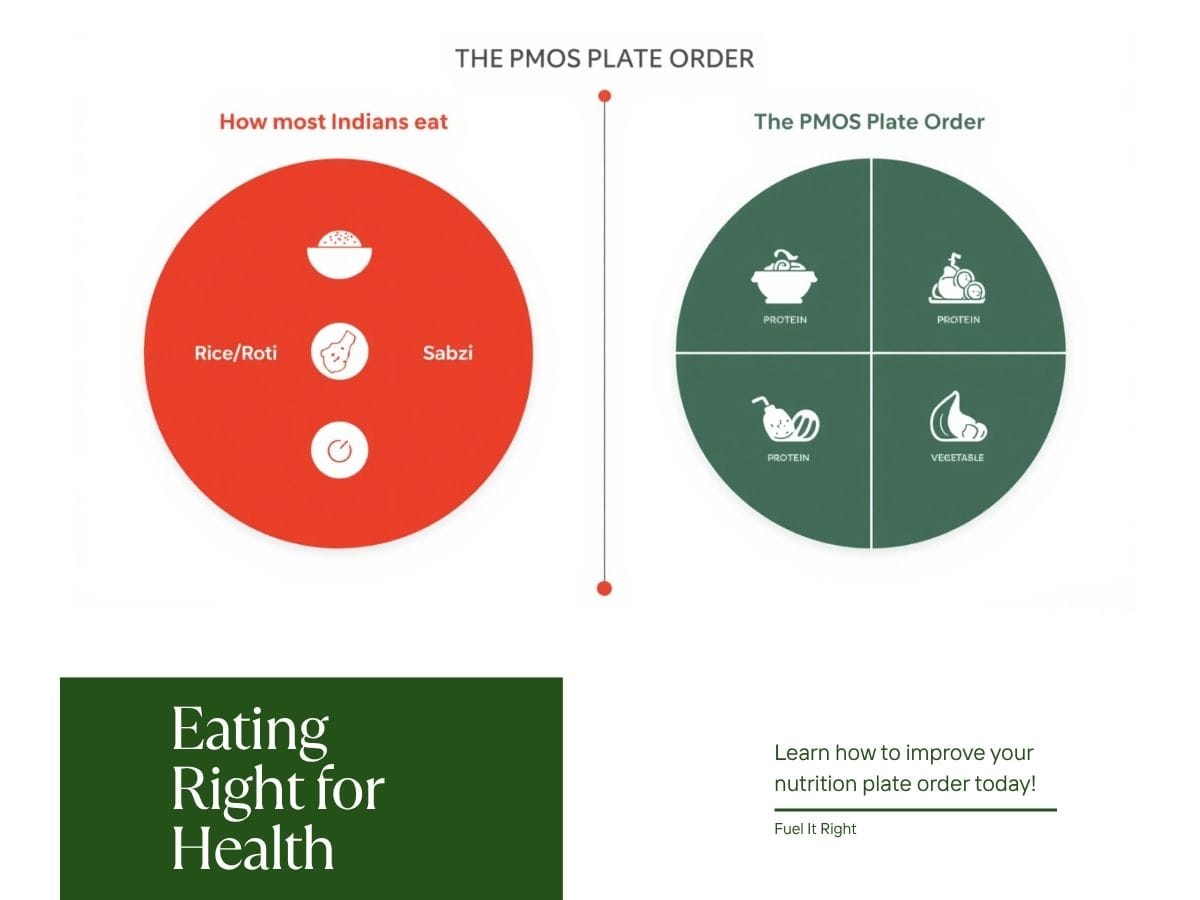
The Principles That Matter
Protein first at every meal: Eating protein before carbohydrates reduces post-meal glucose spikes by up to 30%. Moong dal chilla before the poha. Eggs before the toast. Dal before the rice. The sequence matters more than the quantity.
Fibre with every meal: Fibre slows glucose absorption and feeds the beneficial gut bacteria that support hormone clearance. Seasonal sabzi at every meal is not optional, it is the mechanism.
Anti-inflammatory spices daily: Haldi, jeera, methi, and ajwain each have clinical evidence for reducing inflammation, improving insulin sensitivity, and supporting the gut microbiome. The Indian spice cabinet is a metabolic pharmacy.
Meal timing: Eating the largest meal at midday rather than at night aligns food intake with the body's insulin sensitivity peak. Late dinners drive insulin resistance regardless of what is eaten.
Curd daily: Live cultures in curd directly support the gut bacteria responsible for oestrogen and androgen clearance. The gut-hormone connection is the most under-addressed aspect of PMOS management.
What the Indian Kitchen Already Has
You do not need a Western diet plan to manage PMOS. Every ingredient the metabolic protocol requires is already in an Indian kitchen. Methi seeds reduce insulin spikes. Dal feeds gut bacteria. Ghee supplies butyrate for gut lining repair. Jeera improves enzyme activity. Haldi reduces inflammatory markers.
The problem is not access to the right food. The problem is not knowing how to sequence it and why it works. That is exactly what the 3-Day Indian Gut Reset walks you through as a starting point.
What You Can Do Right Now
PMOS is a metabolism problem and that means there are concrete, food-based actions you can take before your next doctor's appointment, before the next prescription, and before another year of managing symptoms without addressing the root.
1 | Get a fasting insulin test Ask your doctor for fasting insulin and HOMA-IR. These are rarely ordered by default but are the most important numbers for understanding how severe your insulin resistance is. Push for them. |
2 | Add a thyroid panel Ask for TSH and free T4 alongside your hormonal panel. If you have PMOS, you need to know your thyroid status, the two conditions interact directly. |
3 | Change the sequence of one meal At your next meal, eat your vegetables and protein first. Carbs last. Do this for one week and notice your energy levels after lunch. |
4 | Add methi seeds to your morning Half a teaspoon of methi seeds soaked overnight in water, taken on waking. Clinical evidence supports their role in reducing fasting glucose and improving insulin sensitivity. |
5 | Take the gut reset seriously Gut health is not separate from PMOS management- it is central to it. Download the free 3-Day Indian Gut Reset guide and try it this week |
Conclusion: The Name Changed. Now the Treatment Must Too.
PMOS is a metabolism problem. Not an ovary problem. Not a fertility problem. Not a cosmetic problem. Understanding this is not a semantic shift, it is the difference between treating symptoms and addressing the condition.
For millions of Indian women who were told to lose weight, go on the pill, and come back when they wanted to conceive, this reframing is both a vindication and an opportunity. The condition was always metabolic. The treatment should have always started with food.
With me, every protocol we build starts at the root, insulin resistance, gut health, inflammation, and hormone balance, using real Indian food. No supplements. No elimination diets. No guesswork.
If you want to understand what PMOS means for your specific body and where to start, book a free 30-minute discovery call. Bring your blood reports if you have them. We will tell you exactly what they mean and what to do next.
Bring your blood reports. We will tell you exactly what the numbers mean and what food protocol to start.
FAQs — PMOS is a Metabolism Problem: Your Questions Answered
Q1. Is PMOS the same as PCOS or PCOD?
Yes. PMOS is the new official scientific name for the condition previously known as PCOS, and PCOD as commonly used in India. The underlying condition is the same. What has changed is the framing: PMOS correctly identifies it as a metabolic and endocrine condition rather than an ovarian one.
Q2. If PMOS is a metabolism problem, why do my periods get affected?
Because the reproductive system is downstream of the metabolic one. Excess insulin drives excess androgen production in the ovaries. High androgens disrupt the follicle maturation cycle. Irregular periods are a consequence of the insulin-androgen cascade, not the starting point.
Q3. I am lean. Can I still have PMOS?
Yes. Insulin resistance is present in 75% of lean women with PMOS. The condition is not a weight condition. It is a cellular condition. If you have irregular periods, acne, hair fall, or unexplained fatigue regardless of your weight, ask for a fasting insulin test.
Q4. What is the most important test to ask for if I suspect PMOS?
Fasting insulin and HOMA-IR. Most doctors order fasting glucose and HbA1c, which can appear normal even when insulin resistance is significant. Fasting insulin directly measures the compensatory hyperinsulinaemia that characterises PMOS. Push your doctor for this test by name.
Q5. Can food really make a difference to a metabolic condition like PMOS?
Food is the most powerful intervention available for insulin resistance. Protein-first meals, high-fibre vegetables, anti-inflammatory spices, curd, and meal timing all directly affect post-meal glucose response, gut microbiome composition, and androgen levels. The research is unambiguous on this.
Q6. Does PMOS go away after menopause?
The reproductive symptoms resolve, but the metabolic risk does not. Women with PMOS have significantly higher lifetime risk of type 2 diabetes, cardiovascular disease, and metabolic syndrome. Managing insulin resistance is a lifelong priority, not just a reproductive-age concern.
Q7. My doctor never mentioned insulin resistance. What should I do?
Ask directly. Request a fasting insulin test and HOMA-IR calculation at your next appointment. You do not need a referral to ask for these. If your doctor is dismissive, consider a second opinion from an endocrinologist or a metabolic specialist.
Q8. How is the PMOS gut connection relevant to my symptoms?
The gut microbiome directly affects how hormones are processed, cleared, and recycled in the body. Women with PMOS consistently show lower levels of beneficial gut bacteria. Rebuilding the microbiome through fibre, fermented foods, and anti-inflammatory eating reduces circulating androgens and inflammation. The gut is not separate from PMOS management.
About the Author
Shradha | Nutritionist & Dietitian. Practising out of Goa, India, with a focus on gut health, PMOS/PCOS, thyroid disorders, and weight management using real Indian food. No supplements. No machines. Just food, and the science behind it.
fuel-it-right.com | @fuelitright